
Cardiovascular disease progression encompasses more than just myocardial infarction (MI), which is a late-stage event. Myocardial injury, however, can occur earlier and often remains undetected for years. Within the cardiovascular biomarker continuum, the detection of myocardial injury becomes crucial as it provides measurable indicators of ongoing injury and risk assessment. High-sensitivity cardiac troponins, such as high-sensitivity cardiac troponin I (hs-cTnI) and high-sensitivity cardiac troponin T (hs-cTnT), enable the detection of low troponin levels in cases of subtle or chronic injury. This article focuses on how investigating these two complementary biomarkers can enhance our understanding of myocardial injury, asymptomatic progression, and its implications for cardiovascular health.
Troponins are proteins inside heart muscle cells (cardiomyocytes) that help control muscle contraction. When heart muscle cells are injured or stressed, troponin proteins leak into the bloodstream, making troponin measurement in blood a key method to detect myocardial injury.5
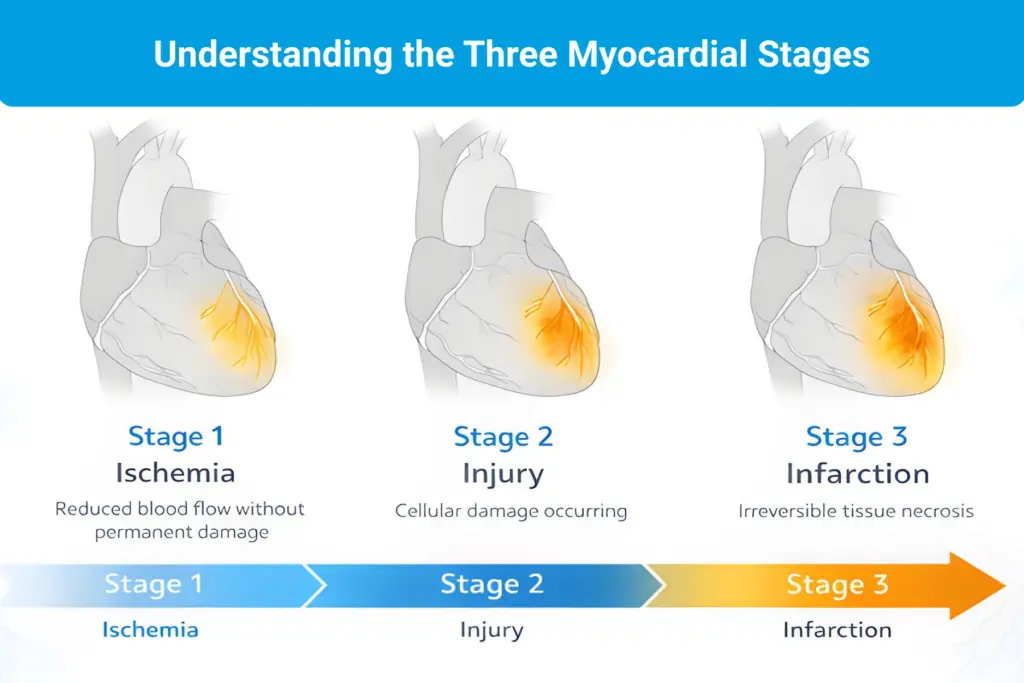
Troponin is often associated with “heart attack,” but contemporary definitions distinguish myocardial injury from myocardial infarction. The Fourth Universal Definition of MI defines myocardial injury as elevated cardiac troponin above the assay-specific 99th percentile, whereas MI requires evidence of acute myocardial ischemia in addition to injury.6
This distinction matters for research because troponin release can reflect multiple biological contexts beyond plaque rupture, including micro-injury, demand ischemia, and structural heart disease. In studies focused on silent progression, hs-troponins provide a measurable signal of injury biology that can be linked to trajectories, subgroups, and downstream outcomes in cohorts followed over time.1–6
In a cardiovascular biomarker continuum model, troponin is most useful as an indicator of injury biology rather than an “MI-only” marker. With high-sensitivity assays, troponin can be detected at very low concentrations, allowing the study of subtle, recurrent, or persistent injury patterns rather than only dramatic, acute events.1–4
This matters because high-sensitivity detection changes the kinds of studies researchers can do. Instead of relying only on event-based endpoints, hs-troponins can be treated as continuous signals that support:
High-sensitivity troponin I and high-sensitivity troponin T both reflect cardiomyocyte injury, but they are distinct proteins measured using different assays. Troponin I is uniquely specific to the heart, while Troponin T is found in heart and skeletal muscles. For research, the practical implication is that concentrations are not interchangeable across platforms. Assay selection and consistency, therefore, matter for study design, especially when subtle injury signals are the focus.2,3
Myocardial injury biology is diverse. Low-level troponin signals can occur in settings where cardiomyocytes are exposed to chronic stress, even in the absence of an acute MI presentation. This supports using hs-troponins to study injury biology across broader populations rather than restricting interpretation to acute coronary syndromes alone.1–6
Examples include:
Within the cardiovascular biomarker continuum framework, the value of hs-troponins measurement lies not only in the ability to detect injury, but also in their capacity to connect injury biology to what follows. Persistent or repeated low-grade injury can be associated with higher future risk and structural change, supporting the use of hs-troponins to investigate progression rather than only acute necrosis.1,4
Myocardial injury is not the end of the cardiovascular biomarker continuum. Over time, injury biology can contribute to remodeling, wall stress, and functional decline. High-sensitivity troponins are essential biomarkers for studying myocardial injury, including subclinical micro-injury patterns, longitudinal trajectories, and outcome linkage in cohorts.1–4
In our next article, we shift from injury biology to cardiac stress and dysfunction. We focus on biomarkers such as NT-proBNP that map to hemodynamic load, remodeling, and progression toward heart failure trajectories. 4,6
No content on this site, regardless of date, should ever be used as a substitute for direct medical advice from your doctor or other qualified clinician.